
Bethune’s Socialized Medicine and the Public Health Crisis Today
“…that consumption and the other pulmonary diseases of the workers are conditions necessary to the existence of capital.” — Karl Marx1
We are at war! The heads of states throughout the globe are posing as chieftains in this quixotic war against an enemy who no one understands. War rooms are being set up to manage data, propaganda, public reactions, and to control supplies, while the foot soldiers – doctors, nurses, other medical and supporting staff – toil to deal with the actual and potential carriers of the enemy, including themselves. Of course, along with them are the baton-wielding workers of the agencies of surveillance – the police, security guards, etc. who are made to assist drones and other AIs to manage the panic and the surplus-ed population (migrants, homeless, and poor) on the streets.
Today, when international and national statesmen are opportunistically posing public hospital workers and those in so-called essential services as ‘warriors’, perhaps it is time for us to understand the reality behind and beyond these spectacular rituals of salutations. For this, we need to pay heed to what Norman Bethune meant when he exhorted his medical colleagues to “organize ourselves so that we can no longer be exploited as we are being exploited by our politicians”2 He too called upon them to engage in a collectivized attack:
“Medicine must be entirely reorganized and unified, welded into a great army of doctors, dentists, nurses, technicians and social service workers, to make a collectivized attack on disease and utilizing all the present scientific knowledge of its members to that end. Let us say to the people – not ‘How much have you got?’ – but, ‘How best can we serve you?’”
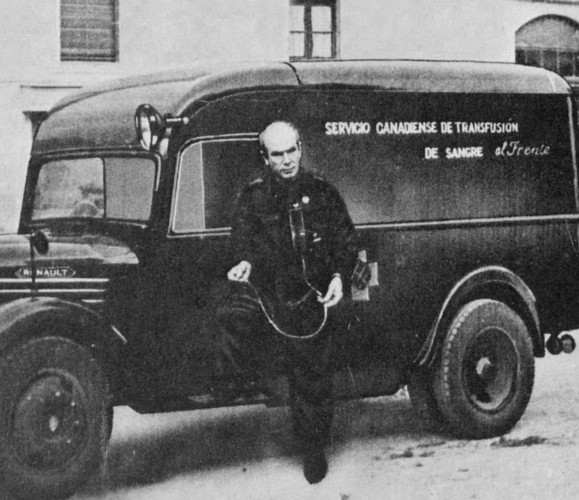
Norman Bethune (1890–1939) was a Canadian surgeon, and a pioneer in the field of thoracic surgery. He was a Communist and an anti-fascist who steeled himself in the Spanish Civil War, fought tuberculosis not just as a doctor but as a patient too, and died in 1939 in the Chinese liberation movement against the Japanese, after getting infected while treating patients without the necessary medical equipment. Norman Bethune was a product of an era that saw the beginning of the industrialization of medicine and medical practices. He made his medical practice a ground for critiquing capitalism and the political economy of modern medicine. We seek to discuss some of his ideas here, and the context in which they were conceived. These ideas gain new meanings in the light of the medical crisis that we face today.
Disease in the History of Capitalism
While the immediate task of controlling the current pandemic determines the actions of states, medical institutions and research laboratories, several critical microbiologists, virologists, and political economists have done well to ask the structural question about the metabolic and ecological rifts that have unleashed new dangers for humanity. They have exposed the truth that “microbes thrive in [the] ‘undercurrents of opportunity’ that arise through social and economic changes, changes in human behavior, and catastrophic events such as war and famine.”3 They have shown how capital in its pursuit to accumulate has eroded species barriers, allowing viruses endemic to particular species to come into contact with humans and domestic animals, leading to antigenic drift and shift. After all, “all progress in capitalist agriculture [and production in general] is a progress in the art, not only of robbing the worker, but of robbing the soil [or nature in general].”4 It is this robbery of nature that perpetuates ecological crises. But, for the ecological crisis to become a ground to rethink structural transformation, it is not enough to locate it in the wreckage that capitalism accumulates. It must be understood as constitutive to capitalist social relations. It is in this sense that the particularization of these crises in the form of pathogens and impending diseases become crucial. This helps us to understand the ecological rift as central to everyday life and struggle in capitalism, and also to imagine transformatory class politics.
Diseases are part of necessary conditions of capital’s existence not only in the sense that they are necessary corollaries of capitalist accumulation but also because they prepare labour for its subsumption by capital for its commodification. In other words, ecological crises through pathogens and diseases give life to capital accumulation by increasing vulnerabilities in social life, creating newer social needs, and thus expanding the scope for capitalist production. History is witness to the role of the second plague pandemic – starting with Black Death of 1348 – in begetting early European capitalism by creating labour shortages leading to technological innovations and the development of the labour market and regulation. Over the centuries, this led to the industrialization of disease management that shaped the theory and practice of medicine and pharmacy.
In the 19th century, when politically coherent challenges to capitalism began to emerge in the labour movement, thinking about the sociological aspects of diseases and their management became crucial to labour. The question of public health became a potent ground for political conflicts. The development of vaccines and medicines, their production and distribution, and the approach and regulation of medical practice were some of the major issues in this regard. Frequent recurrence of epidemics and pandemics, along with colonization and wars, and the emergence of strong anti-capitalist revolutionary movements in the 20th century led to the emergence of radical approaches in every field of knowledge, including medicine. Norman Bethune was a product of this era.
Capitalism and Medical Economics
During the current age of pandemics, we suddenly realize that we are part of the same humanity, despite all kinds of exclusion that surround us and our lives. Instead of accepting this togetherness as a necessary characteristic of our species existence, and thus acting according to our nature, we struggle hard to shield ourselves against it – thrusting toward extreme self-alienation. Capitalism is founded on individualism and competition, leading to an unquenchable thirst for private appropriation, which is actually a shield that makes us appear exclusive, beyond the reach of other beings – humans or non-humans. But this shielding is possible only by evermore socialization of production (mass production, through human cooperation), which is the basis of technologically advanced and sophisticated commodity production. The continuous pull-apart between social production and private appropriation, which is the defining contradiction of capitalism, creates frequent glitches in the form of overproduction, underconsumption, and overaccumulation, leading to full scale, severe economic crises. These crises in themselves constitute, as Norman Bethune puts it, “a deadly disease,” requiring “systematic treatment,” not palliative measures from “our political quacks,” which are like “aspirin tablets for syphilitic headache.”
According to Bethune, after the industrial transformation that happened in the 19th century, private health ceases to exist, since maladies and maladjustments of one section affect other sections of the masses as well. In this sense, all health is public health. What we witness in frequent epidemics since the early 20th century is a continuous reaffirmation of this fact in their expanse and velocity, while some diseases with relative virulence and communicability such as tuberculosis continue to remain necessary conditions for the existence of capital. But, alongside the socialization of disease and scientific abundance, the appropriation of health resources and services has become more and more privatized.
It is in this regard that Bethune talks about the problems of medical economics – of millions being sick, in pain, and hundreds of thousands dying prematurely due to inaccessibility to adequate and timely medical care. But this problem is part of the problem of world economics, “of selling bread at the price of jewels,” of practising medicine as a “luxury trade,” of commodification, and thus, of capitalism, itself. Because of its inseparability from and embeddedness in the social fabric, medicine, today, “is a typical, loosely organized, basically individualistic industry in this ‘catch as catch can’ capitalistic system, operating as a monopoly on a private profit basis.” And, thus what happens to capitalism in general happens to this industry. Along with other sectors of economy, this industry too faces economic crises.
Bethune identifies the chief contradiction of medical practice ensuing from its embeddedness in the capitalistic industrial processes. On the one hand, medical knowledge (and scientific knowledge) has become so enormous that individualistic medical practice has become an impossibility. On the other hand, this same fact leads to specialization, which, in the context of industrialization and commodification of medical education, is kept out of reach for the majority of medical aspirants. Consequently, the pecuniary logic (“fee-for-service”) is instilled into the very work process of medical practice in capitalism, which Bethune finds morally very disturbing.
The way medicine was organized as a discipline and practice affected the approaches to diseases too, thus raising important epistemological issues. Bethune was dissatisfied with the prevalent approaches to pulmonary tuberculosis because they took an attenuated viewpoint of the disease, focussing on nothing but the local pulmonary lesion. According to Bethune, curing this disease required a holistic approach toward the infected individual – as a product of his social and physical environment – and, with the tubercle bacillus as just another factor in the environment of man, causing bodily and behavioral changes. He said,
“Any scheme to cure this disease which does not consider man as a whole, as the resultant of environmental strain and stress, is bound to fail. Tuberculosis is not merely a disease of the lungs; it is a profound change of the entire body which occurs when man, regarded as an organism acting under the dictation of, and the product of, his environment, fails to circumnavigate or subjugate certain injurious forces acting on his body and mind. Let him persist in continuing in such an environment and he will die. Change these factors, both external and internal, readjust the scene, if not the stage, and he, in the majority of instances, will recover.”5
It was this recognition of the mutual embeddedness of economics and pathology that defined Bethune’s unconventional life and work as a surgeon, and transformed him into a revolutionary. The practice of socialized medicine, as he conceptualized it, was not simply a demand on the state and doctors, but was, rather, a dimension of transformatory politics translated in the field of healthcare.
Socialized Medicine
 It is through a critical (self) inquiry into the theory and practice of medicine that Bethune develops the conception of socialized medicine. For Bethune, there is a continuous ideological class struggle going on within the field of medicine. On the one hand are those with allegiance to individualism – reactionaries represented in medicine by those who uphold private property and monopoly of health distribution. On the other hand, we have those who envisage and engage in cooperative efforts for the betterment of one and all.
It is through a critical (self) inquiry into the theory and practice of medicine that Bethune develops the conception of socialized medicine. For Bethune, there is a continuous ideological class struggle going on within the field of medicine. On the one hand are those with allegiance to individualism – reactionaries represented in medicine by those who uphold private property and monopoly of health distribution. On the other hand, we have those who envisage and engage in cooperative efforts for the betterment of one and all.
According to Bethune, changing the economic system that breeds ill health, ignorance, poverty and unemployment is the only guarantee for providing universal health protection. He considered socialized medicine as a negation of this system in medicine. This concept, however, cannot be reduced to medical reforms like health insurance schemes, which are essentially based on the commodification of medicine and the establishment of an entire industry around it. Bethune considered these reforms to be “bastard forms of socialism produced by belated humanitarianism out of necessity.” In fact, for him, philanthropy and charity have kept the outmoded and wasteful private practice in medicine alive. They must be abolished, since “charity debases the donor and debauches the recipient.” They rob the public of their right to health protection.
If there is no private disease, there cannot be private health protection. Bethune called for the abolition of individual selling and purchasing of medical care. His conception of socialized medicine envisaged an overhauling of the foundation of bourgeois medicine by considering health protection a public property that must be supported by public funds. The administration of health services must be need oriented – to each according to his needs. It calls for a revolutionary transformation by calling for a bottom-up “democratic self-government [of healthcare] by the health workers themselves.”
Bethune made a scathing attack on those who defended private practice and opposed socialized medicine in the name of individualism, incentive, choice, and bureaucracy. He called for redefining “medical ethics – not as a code of professional etiquette between doctors, but as a code of fundamental morality and justice between medicine and the people.” According to him, medicine and public healthcare need a holistic approach toward diseases, taking patients to be products of their social and physical environments. Hence, more than famous personalities, healthcare requires far-sighted, socially imaginative leaders and statesmen in medicine who are not just looking for interesting cases but seek to provide a collectivized attack on diseases, for which an understanding of the relationship of medicine with the larger society, state, and economy is necessary. Socialized medicine is a collective practice of delivering socially comprehensive and lasting results, rather than providing private service to people who can afford it. It is a challenge to the subsumption of medical labour by capital and a reclaiming of knowledge by humanity at large.
The Context of COVID-19
A disease is not an epidemic or a pandemic unless it is recognized as such, and this recognition is only partially determined by its biology. Of course, the suddenness and extent of death, and the engendering of fear are its necessary aspects. However, the trajectory of its spread, the nature of public reaction, and the way it is interpreted are mainly determined by non-biological factors such as the physical environment, socio-economic relationships, political structures, social attitudes, and intellectual-cultural atmosphere. An American historian of medicine Charles Rosenberg, based on his reading of Albert Camus’ The Plague, underlined the episodic nature of epidemics eliciting a spectacular response. He considered an epidemic to be a social phenomenon which unfolds in a dramaturgic form, with progressive revelations, engendering individual and collective crises, and then drifting toward closure.6
Unlike earlier experiences, with COVID-19 we see an emergence of the whole world as a stage where the drama unfolds. This is, of course, due to the technological shrinkage of time and space in our age – now, microbes take flight. But the spectacular similitude of crises and responses at this level demonstrates how social structures, ideologies, and social values have converged globally. The rhetoric of war and the institution of quarantine, where everyone is a warrior, a victim, and a suspect at the same time, have mobilized individuals and communities to act out rituals that affirm bellum omnium contra omnes (the war of all against all), the foundation of capitalism.
Today, agencies world over are paying tribute to the medical warriors who are fighting at the frontlines of the war against COVID-19. Financial incentives and benefits (sometimes to be accorded posthumously) are announced for these soldiers, world leaders fill their speeches with plaudits for them, and local citizens applaud them with the rhythmic chimes of bells and claps. Sometime in the future, the war will be over. The warriors will be back at their old posts in a ‘new normal’ world. This ‘new normal’ to which we will return will be the ‘normal’ tenfold more severe in alienation and individualism. This is the world that we have prepared ourselves for in the last few months through corporeal and mental self-isolation, and by the technologically-secured globalized institution of quarantine.
Some voices today are celebrating the possibility of a return to state socialism and welfarism, but the stronger tendency is toward a congealment of a technologically sophisticated global-surveillance capitalism, overseen by the state, based on real and manufactured panic of self-obsessed alienated individuals and their competitive survivalism. This is, of course, not an atmosphere conducive for a strong public health system but, rather, for reckless private appropriation of health resources – which will be the ground for further corporatization of medicine and health industries.
Bethune’s concept of socialized medicine was a product of the era when liberal capitalism was on the verge of collapse, and a national consolidation of labour and resources was sought everywhere. Thus, in Canada, for instance, this concept was reduced to policies of state-run healthcare. But the fundamental aspects of this concept could never be exhausted in the instrumentality of policy measures and temporal demands. Its epistemology, the critique of capitalism and the notion of medicine as social practice geared toward a radical restructuring of the society, where knowledge is the power of – not over – the human, are the insights that need to be mobilized today to challenge the global consolidation of state and capital in the age of emerging viruses. •
Endnotes
- Karl Marx (1976) Capital. Volume 1, (Trans. Ben Fowkes). London: Pelican Books, p. 612.
- All quotes, unless numbered, are taken from Norman Bethune’s 1936 speech at a panel discussion on economic problems of medicine organized by the Montreal Medico-Chirurgical Society, reproduced in Sydney Gordon and Ted Allan’s (1952, 1973) The Scalpel, The Sword: The Story of Norman Bethune, Monthly Review Press, pp 92-98.
- Richard M. Krause (1993) Foreword in Stephen S. Morse (ed.), Emerging Viruses. Oxford: Oxford University Press.
- Karl Marx, op. cit., p. 638.
- Norman Bethune (1932) “A plea for early compression in Pulmonary Tuberculosis,” The Canadian Medical Association Journal, 27(1), 36-42. Retrieved May 17, 2020.
- Rosenberg, C. (1989). “What Is an Epidemic? AIDS in Historical Perspective,” Daedalus, 118(2), 1-17. Retrieved May 17, 2020.



