
Alberta is Privatizing Healthcare: Threatening Public Healthcare Across Canada
Alberta’s government, led by Danielle Smith and the United Conservative Party, passed a new law, Bill 11: The Health Statutes Amendment Act, last week. With its passage the existential threat to public medicare in Canada is here. The new law sets up two-tier medicare and private health insurance in Alberta. It is terrible for Albertans, destroys single-tier public medicare in Canada as a national achievement, and puts at threat public healthcare across the country. It follows on the heels of the Alberta government’s repeated use of the Notwithstanding Clause to enable violations of the Canadian Constitution and Charter of Rights and an emboldened push for Alberta’s separation from Canada among some forces in the province.
This attack on public healthcare threatens all of Canada. It would be naïve, indeed, to believe that private insurance companies will stop at the Alberta border. Moreover, the trade agreements carve out public healthcare only so long as it is public. The new law is an abrogation of our national values and the beliefs that we hold dear: that Canadians should take care of one another, that we believe in equity and compassion, and that judge and janitor would have an equal interest in a high-quality public health system because access to care would be based on medical need, not how rich you are.
It is hard to overstate how destructive this legislation is.
For those who want to understand the basics, please see the overview, note on manipulative language and the consequences sections below. For those who want more details about the actual legislation and how it works, please see the analysis of the Act further below.
I hope this article is helpful to understand what is happening. Clearly, we need a Canada-wide fightback commensurate to the threat. We are working on that now.
Thank you,
Natalie Mehra
Executive Director
Ontario Health Coalition

Overview: What We Currently Have
The Canada Health Act requires provinces to provide all medically necessary hospital and physician services under public health insurance. It is like a bill of rights for patients. Canadians have the right to medically necessary hospital and physician care on equal terms and conditions, without financial barriers. Extra-billing patients and charging user fees for medically necessary hospital and physician services are banned. In plain language, you cannot be charged for a doctor’s visit, a medically needed diagnostic test, a surgery or a medically needed procedure, whether it is in a public hospital or private clinic or doctor’s office. (Note: they can legally charge for medically UN-necessary things and some provinces have delisted some procedures, and these have sometimes wrongfully been used to push the boundary. Nothing comes close to what Alberta is doing right now, however.)
Each province has a public health insurance plan that is required to cover medically necessary hospital and physician care. The public insurance system in Ontario is called OHIP. In Alberta it is AHCIP, in BC – MSP, Quebec – RAMQ, and so on. This refers to the public health insurance system.
Our healthcare is single-tier, meaning that all Canadians have equal access to care based on your medical need not wealth. It is a national standard across the country and a celebrated part of what it means to be Canadian.
The provinces are required to abide by the Canada Health Act. The federal government is required to claw back funding if they allow patients to be charged for needed healthcare. This protects patients from the suffering and poverty that led to the creation of public healthcare in our country and that so many people experience in the United States.
In the provinces, physicians have an interest in staying in public healthcare because: a) they are doing incredibly well by it (they are generally in the top 1-2% of income earners), b) they have ethics and support public access to healthcare, and; c) if they don’t want to be part of public healthcare, they have to completely opt out of public healthcare and not bill the public health system to charge for private care. (Note: Under Ontario law, physicians cannot opt out at all and in other provinces there are public protections and barriers to it.) Thus, there is a barrier to opting out and in most provinces only a tiny proportion of physicians have done so. They would have to believe they could create an entire practice of privately paying patients and be able to earn as much money or more from it.
In sum, the protections that Canadians currently have to protect single tier public healthcare are the following:
- the public health insurance system has to be publicly administered and non-profit (thus, operated in the public interest not for private profit-seeking interests);
- it has to cover medically necessary hospital and physician services;
- all Canadians must have reasonable access to medically needed hospital and physician care on equal terms and conditions and without financial barriers, whether direct or indirect;
- extra-billing and user fees are prohibited, and;
- physicians are either not allowed to opt out (as in Ontario) or have to opt out entirely and not bill the public health system in order to bill patients privately.
Together, these things protect us from US style private for-profit healthcare.
Why Does it Matter?
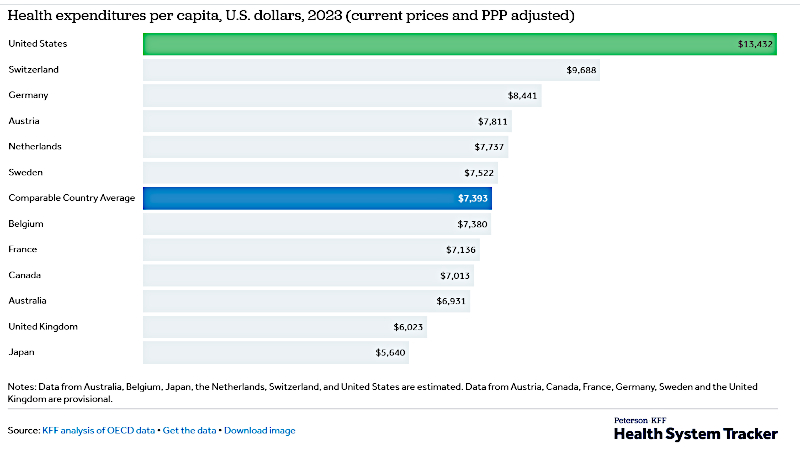
Public healthcare is far less expensive than private healthcare. Americans do not realise that they pay almost double what Canadians pay for healthcare. Even after charging far more, private insurance companies require US patients to pay deductibles before they get coverage, deny claims, and tie patients up in red tape. Private health insurance is inequitable… deeply inequitable. It changes a society entirely. In Canada, we often talk about economic issues as being the actions of private industry. In the United States, everyone understands healthcare to be a major economic issue, and medical bills are a leading cause of bankruptcy.
Public healthcare advocates work to protect, improve, and expand public healthcare because public healthcare is less expensive, reduces suffering and inequities, and supports people to live dignified lives, and because we fundamentally believe that in a good society we take care of one another. Physicians and health professionals who support public healthcare do so because it means the practice of medicine is ethical and serves the public interest. It is not focused on taking profit but rather on providing care and treating patients.
What Alberta is Doing
With their new law, Alberta has brought in private for-profit health insurance. It is not an exaggeration to call that US-style. It is indeed US-style private health insurance and two-tier healthcare. It is unprecedented. It wipes out equal access to care based on medical need, not wealth. It wipes out the prohibition on both charging patients and charging the public health system. There are no price controls and any protection of equality is rendered meaningless.
The new law is written to remove the barriers to the creation of a “market” for private health insurance. That is the purpose. Under it, doctors can charge both the public health system (AHCIP – equivalent to Ontario’s OHIP) and charge patients directly, and they can jump back and forth at will. It explicitly sets up private health insurance, and doctors will decide which patients to stream into private payment and for which items. (More details on these provisions below.) Thus, the public system will be the safety net while they build private healthcare.
Purposefully Manipulative Language to Make the Extreme Sound Moderate
A quick note about language. It is disturbing to see the media coverage and commentary about this new law. A lot of it uses words like “dual practice,” “hybrid,” “public and private.” Anything to avoid saying “two-tier healthcare” or “privatization.” Their language is both confusing and fails to capture the main intent. The clear goal of the legislation is to set up a market for private health insurance and to direct charges to patients, and with it, two-tier healthcare. There are entire sections of the legislation that serve no policy goal and run counter to the public interest, except that they make it easier to bring in and expand private healthcare and develop a market for the private health insurance industry.
Please remember that the framing of this issue has long been planned by the forces that want to dismantle and privatize public medicare in Canada.
For example, in November 2005, Brian Day – owner of a large for-profit clinic in BC – hosted a “Saving Medicare Summit” in Vancouver. (Day went on to launch a legal case in which he attempted to bring down the laws that stop two-tier healthcare in British Columbia. He lost at every level in the courts.) The conference openly advocated full two-tier medicare. Given the framing in the media and commentary right now, it is timely to remind ourselves that at that conference, Preston Manning, founder of the Reform Party, recommended the delegates to:
Present their ideas as a “compromise”: “Canadians love compromise.” Redefine two-tier medicare as between the status quo and the US private system. Make the extreme seem moderate. Make the proponents of public healthcare seem extreme.
“Once the battle over language has been won,” Manning said, it will be politically easier to follow its substantive prescription: completely dismantle national Medicare, have the federal government hand over more taxing power to the provinces and let them handle Medicare as they please.

To really get a sense of how deliberate the plans and how carefully selected the language used to sell them and overcome Canadian resistance to privatization, here is an article quoting their strategies in their own words.
Consequences of the Alberta Legislation
- Alberta’s new law brings in US style private health insurance, including workplace plans. They will not stop at the Alberta border. This legislation will feed a market of private health insurance that will use every method they can to expand across Canada.
- It threatens public healthcare in Alberta and across Canada, and it violates our core values of equity and compassion. Healthcare will no longer be provided equally to executives, farmers, the middle class and the working class. It will be provided based on who can afford it and those whom private health insurance companies will cover.
- It threatens Canadian sovereignty, ending national public healthcare which is foundational to our uniqueness and difference from the United States.
- It threatens single-tier public medicare across Canada by making health insurance private, thus no longer protected from trade agreements with the United States. As long as our health insurance is public, we can stop US private health insurance from moving in. When that is gone, and we don’t know exactly what is the tipping point, we no longer have the carve out.
- It will cause a sharp escalation in prices and costs for healthcare services. In the US, private insurance and out-of-pocket costs are extremely variable and are very high across the board, often many times the cost for diagnostics, treatments and procedures in Canada. European countries with private health insurance also have higher costs than we do.
- It will cause gross inequities and loss of access to public healthcare, favouring high income earners, large urban centres with a profitable “market” of private pay patients, and younger and healthier people who private health insurance companies see as profitable. It will cause a loss of services for the elderly, those with chronic health conditions and ill health, everyone who cannot afford the high cost of private health insurance and out-of-pocket charges, rural communities and the north, among others.
- Costs will increase for employers and will be passed on through co-pays and deductibles to employees also. Employers will face new private health insurance costs. The experience from the US is that on top of new costs for employers, employees will face deductions from payroll to pay for health insurance, and on top will have deductibles. When employees lose their jobs, they lose their health insurance.
- Unions will be pressed into bargaining for health insurance coverage and that will replace wages, pensions and other benefits.
- It will seriously impede, if not make impossible, sound planning for the provision of public healthcare services as physicians can move back and forth between public and private without time delays.
- Staffing shortages for public healthcare will worsen, compounding the gross inequities created by private health insurance.
- People will have to pay for healthcare both through taxes and private payment. It is an added cost, not a cost reduction.
Analysis of Alberta Healthcare Insurance Act Amendments
Here is a quick summary and analysis of the main changes.
1. The changes set up three categories of physicians and two categories of dentists:
- Participating physicians who provide insured health services (AHCIP, which is Alberta’s equivalent to Ontario’s OHIP, Quebec’s RAMQ, or BC’s MSP).
- “Flexibly participating physicians” who provide insured health services (AHCIP) and privately insured services
- Opted-out physicians who provide only privately insured services
- For dentists the changes create two categories – those in and those out. They do not include the “flexibly participating” in – and out at the same time – category.
- Specific changes to opted in and opted out dentistry run throughout the Act but I am not covering them here. I am focusing only on public healthcare services.
These changes mean that physicians can provide publicly insured (AHCIP) health services, or they can opt out entirely, or they can both bill the public plan and charge privately.
Prior to this, Alberta physicians had to be in or out. If they opted out, they couldn’t bill the public health system (AHCIP). This was a protection for the public system, ensuring that most physicians would stay in the public system and thus Albertans’ access to care would be protected because opting out entirely would be risky and would make it harder to make a good income. (To do so they would have to make an entire practice from the small “market” of wealthy executives to make their entire income.) Notably, physicians have been among the prime beneficiaries of public medicare. They have very high incomes under our public healthcare system without any extra user charges. Across Canada, doctors are in the top 5% of income earners in every community and many, if not most, are in the top 1-2%. Those who want to charge more want to make more than they are currently.
2. The changes also set up private workplace health insurance plans for current and former employees. This is notable and appears to be one of the main goals, if not the main goal, of this legislation.
3. In order to opt-out or be both in- and out- (i.e. a “flexibly participating” physician) the physician must notify the Minister of Health in writing. The Act specifies that physicians can go back and forth, meaning they can jump in and out of the public insurance system entirely, or jump into and out of being “flexibly participating,” as they wish at any time and without any delay. To do so, they simply have to notify the Minister in writing. However, in the Act, they expressly do not have to tell the Minister what services they are providing under public insurance and what services they are selling privately.
The implications of this are significant because it means the Minister would lose the ability to gauge what public healthcare services are being delivered and where. Since physicians can jump back and forth after simply sending a notice to the Minister, those services would be subject to significant variability at any time, making it much more difficult – if not impossible – to plan for equitable and sufficient public healthcare services. Furthermore, private health insurance indisputably creates inequities and the ability for the Minister to reduce those is severely limited by the way they have written this bill.
The Alberta government has tried to deal with the obvious problems of gross inequities created by this plan by adding in clauses that enable the Minister to restrict which services can be sold by opted-out and “flexibly participating” physicians and by setting conditions, circumstances, restrictions, and other controls over what services can be sold privately. These clauses are insufficient to counter the fact that they have expressly allowed physicians not to tell them what services they are providing inside and outside the public health system and to jump back and forth at any time without delay. People would have to raise a hue and cry over poor access to care, and force the Minister to take action. Given how much this legislation is slanted in favour of the private insurance industry and physicians who want to charge (higher) prices privately, it is not clear how inequitable the situation would have to get to force the Minister to take action. (We have to understand, the legislation purposely sets up an inequitable healthcare regime. Thus, the Alberta government anticipates tolerating a level of inequity that we have never seen before.)
Why would they not require physicians to pre-register what they are going to privatize and subject it to oversight before-the-fact or impose delays to jumping in and out of the public insurance system? All of this is explained by the next change (listed below). The goals appear to be to create a private health insurance market and to enable physicians maximum flexibility to move into and out of it with little risk. This legislation does not reflect the public interest in health planning or in improving access to care. It reflects the interests that want to remove barriers to creation of a private health insurance market by removing the risks. It creates easy pathways of entry into the private market for physicians with the ability to go back and forth at will without even notifying the Health Minister of which particular services the public system will be providing until the Minister collects records after-the-fact.
Nowhere does it say that a patient has the right to informed consent about whether or not a physician wants to charge them or bill the public plan. The choice is left up to the physician alone. (If a patient can’t pay, they have to go without or go elsewhere, but the choice about which stream to put the patient is the doctor’s, under this law.) Patients are not at the centre of this Act, in fact, quite the opposite.
In addition, the Minister is restricted from issuing orders, restrictions, conditions, etc. on what services can be privatized by a clause saying that they must give 90 days notice to physicians unless the Minister deems it appropriate or necessary for the adequate provision of health services.
It is reasonable to conclude from these policy choices that the Act was written for the private health insurance industry and physicians who want to bill both the public system and privately with impunity and without risk.
4. A “flexibly participating” physician may decide on a case-by-case basis whether to provide a service described as a non-plan (i.e., privately paid) or covered (AHCIP) service. Thus, the physician determines whether they want to charge the patient or not and when.
The patient does not have the right to choose whether they get public coverage – nor for which services – with that particular doctor. Under the changes in the Act, the patient must simply be notified of the physician’s choice to have the patient pay, the nature of the service that is subject to private payment, how much the patient is required to pay, that the patient cannot get reimbursed by the public system (AHCIP) for that service, and that they can go elsewhere to try to find a physician who will charge the public system (AHCIP). The physician is required to have the patient to sign off on the agreement to pay and the amount. If the patient will not sign off, they would have to go without the service or try to find another doctor who won’t charge them.
The physician cannot charge both the public system (AHCIP) and the patient (i.e. extra bill the patient) for the privately-paid service. The physician cannot charge user fees as a condition of receiving a publicly insured service (AHCIP). This appears to be a nod to the Canada Health Act, which bans user fees and extra-billing. It is dubious whether Alberta will start enforcing these provisions. In any case, they are bringing in entire private health insurance and private payment, so doctors can charge patients directly for medically needed services. Whatever equality effect the ban on user fees and extra-billing had under a public insurance system is completely destroyed by private health insurance. Moreover, the Canada Health Act was written to ensure that Canadians be provided healthcare on equal terms and conditions and without financial barriers. Obviously, this legislation destroys any right to equality in access to healthcare.
To enable these provisions (above), the Act makes related changes to health cards, billing enforcement, health information sharing, and hospital/agency statutes. •



