
Ontario’s Healthcare Capacity Crisis: Ford Government Plans to Make It Worse
Despite the current healthcare capacity crisis, the Doug Ford government in Ontario plans to cut healthcare service levels.
Hospitals: The news is bad for hospital services. The new Financial Accountability Office (FAO) report on the government’s healthcare funding plan reveals that the government plans 3,000 new beds over the next decade – that’s about an 8.4% increase in capacity. Measured against need, however, this will mean a sharp decrease in service levels. The public wants improved service levels, but the opposite is planned.
That ‘increase’ won’t come even close to covering the increasing demand for services due to population growth, which according to provincial government projections will be about 15%. The demands on healthcare will be much more than this, however, due to a rapidly aging population.
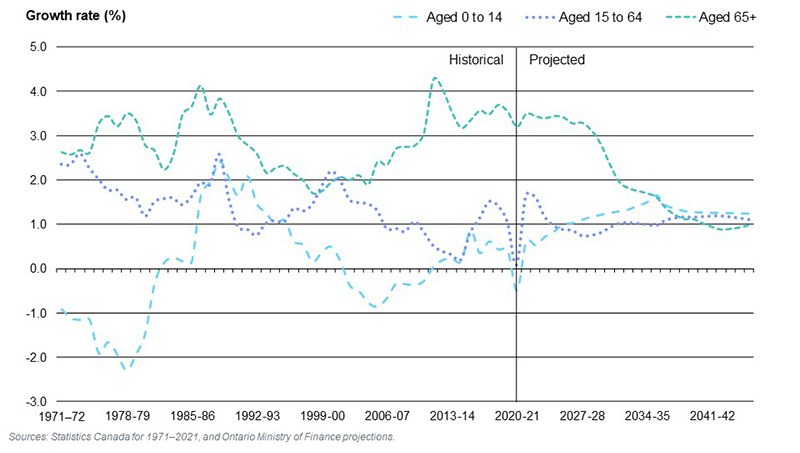
Healthcare needs are very sensitive to age. People 65 and over use most of our hospital bed days – 58% in 2018/19. The population of the 65+ age group is projected to grow by close to 3% a year, twice the rate of the overall population. We will have about a third more people aged 65+ in a decade. According to the Ontario Ministry of Finance projections, the oldest segments of the 65+ age group (the 75+ and 90+ age groups) are projected to grow the fastest, compounding the need for extra hospital capacity.
The rapid growth in the number of elders is driving up the need for hospital beds (and the hospital workers to staff them) by more than double the planned increase in staffed beds. Aging is a long-term trend and should have been planned for decades ago, but capacity was not adjusted for that reality, and the result is this predictable crisis that should, at the very least, be planned for now.
Pace of growth of population age groups 0-14, 15-64 and 65+ in Ontario, 1971 to 2046
The present plans for the years immediately ahead are wholly inadequate. The FAO estimates that, despite the current capacity crisis, only 1,000 new beds will be added in the next four years, less than a 3% increase. That’s enough for about two years of population growth, with nothing to offset aging, much less improve service levels and deal with the capacity crisis.
The plan is to double down on long-term cuts in hospital-service levels – a very funny way to respond to a hospital capacity crisis. Hospital-service levels are going to take a plunge unless the Ford plan is changed and more capacity is added.
Homecare: A similar dynamic plays out in homecare. The government trumpets new money for homecare – but (with aging and population growth) the FAO projects a decline in the number of nursing and personal support hours per Ontarian aged 65 and over, from 20.6 hours in 2019-20 to 19.4 hours in 2025-26. That is down 5.8% – almost 1% per year. Unless this improves, there will be no relief of the pressure on healthcare through homecare – in fact, just the opposite.
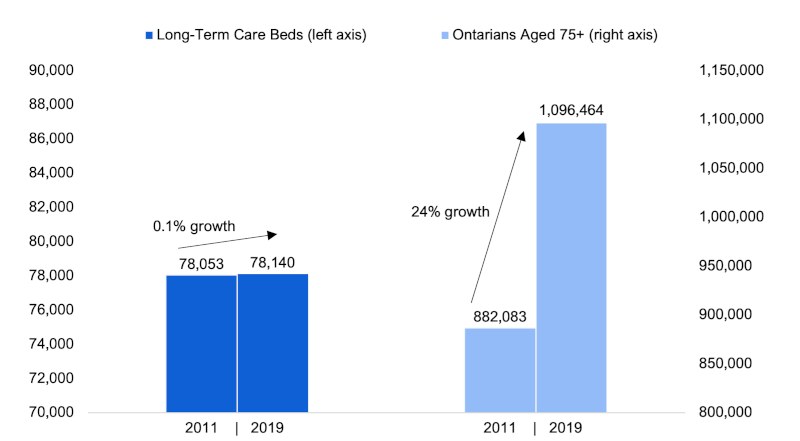
Long-Term Care: There was one small bright spot in the Financial Accountability Office’s report on the government’s healthcare funding plan. But it’s a very tiny one, and only if you ignore longer-term cuts.
The FAO now sees a slight improvement in the ratio of long-term care bed to elders 75 years of age and over – from 71.3 beds per 1,000 in 2019-20 to 72.1 in 2027-28. The increase amounts to a 1.1% increase over 8 years. That’s an increase of 0.1% per year.
How is this the plan when almost 40,000 elders are on the LTC wait list and the government has just passed legislation to coerce hospital patients to move into long-term care? Even with this very modest increase, we are still far short of the 90 beds per 1000 elders 75 and over in 2010/11 – 20% less.
Like hospital-bed capacity, the need to improve LTC bed capacity has been long ignored by governments , despite the obvious growth in the elder population. Ford’s plans to build new capacity in LTC only very modestly improves the low level of capacity established over the last 20 years, during which governments decided to all but stop the creation of new LTC beds.
So, this may be better than nothing – but an improvement? That’s a stretch. We are far behind where we were only a decade ago.
Surplus healthcare funding? The media focused on $4.4-billion “more than what is necessary” in planned healthcare funding reported by the FAO over four years.
But the FAO was not measuring funding against need – it was measuring funding plans against these miserable service-level plans developed by the provincial government. It’s not hard to have a surplus when you are actually cutting service levels. And in any case, with the final defeat of the government’s unconstitutional Bill 124, the FAO estimates that an additional $2.7-billion will be needed to provide higher hospital wages than it had forecast through 2027/8 (on top of the $900-million already bargained-for higher wages under the Bill 124 period).
The bottom line is that the government is planning 3.9% annual healthcare funding increases from 2021-22 to 2027-28, and no one can credibly claim that is sufficient to keep up with rising demand. Even before the current wave of inflation, healthcare cost pressures were commonly put at over 5% per year.
Despite the capacity crisis now driving unprecedented hospital closures, the plan of the Doug Ford government is to cut service levels further. We are in for a decade of trouble unless this changes.
In 2018, Ford ran on a promise of ending hallway healthcare: now more inpatients languish in hallways than ever, hospital ERs are closing, and staff vacancies have sky-rocketed.
Now we know the response is to cut capacity relative to rising need. •
This article first published on the Defend Public Healthcare website.



